BLOG

You had veneers or crowns done in Turkey. The photos looked good on the day. But now — a few weeks or a few months later — something feels off, and you're searching to find out if that's normal or if your treatment was botched. This guide walks through exactly that: the difference between expected healing and a genuine warning sign, what causes each problem, and what an honest fix actually looks like.
| 9/10 UK dentists have treated complications from dental work done abroad (BDA) |
2–8 Weeks after treatment is when most genuine problems actually surface |
2 Main types of failure: over-prepared teeth, and rushed/mismatched fit |
"Botched" gets used loosely online, and that makes it harder, not easier, to work out where you stand. There is a real difference between not loving the shade or shape of your new smile — a cosmetic preference that a dentist can usually adjust — and a clinical problem that will get worse if it's left alone. This article is about the second category: pain that persists, gums that won't calm down, a bite that doesn't sit right, restorations that are visibly failing.
Most people who search for this term went in expecting veneers — thin porcelain shells that need only a sliver of enamel removed — and came out with full crowns on every tooth instead, often without a clear explanation of the difference. A veneer covers the front surface of a healthy tooth. A crown covers the entire tooth and requires the tooth to be reduced down to a smaller core first — sometimes to a small peg — to make room for it. When a patient says their teeth were "filed down to nothing," they are almost always describing crown preparation that they did not know they were getting. This single mix-up is behind a large share of the complaints associated with "Turkey teeth."
| The key distinction: A veneer needs a healthy tooth underneath. A crown replaces most of the tooth's visible structure. If you asked for one and received the other without being told, that is the root of most "botched" complaints — not necessarily the skill of the dentist. |

Some discomfort right after treatment is normal, not a red flag. Mild sensitivity to hot, cold, or pressure is common while the tooth and gum adjust to new restorations. Gums can look slightly pink or puffy around the margins for the first week or two, especially if several teeth were prepared close together. Getting used to a new bite — teeth meeting at a slightly different angle — can feel strange for a few days. None of this, on its own, means something went wrong.
By four to six weeks, initial healing should be settling, not worsening. If sensitivity is the same or worse than week one, if gums are still bleeding on brushing, or if you're noticing a persistent bad taste or smell, it's worth having a dentist look — not because it's necessarily serious, but because problems caught early are far easier to correct than problems left to progress.
Symptoms that appear or worsen months after treatment are the clearest signal that something structural is wrong, rather than the tooth simply still settling in. A tooth that starts throbbing or darkening months later often means the nerve was affected during preparation. Gum recession that exposes a dark line at the edge of a crown, or crowns that begin lifting or separating, point to a fit problem rather than normal wear. These are the signs covered in detail below.
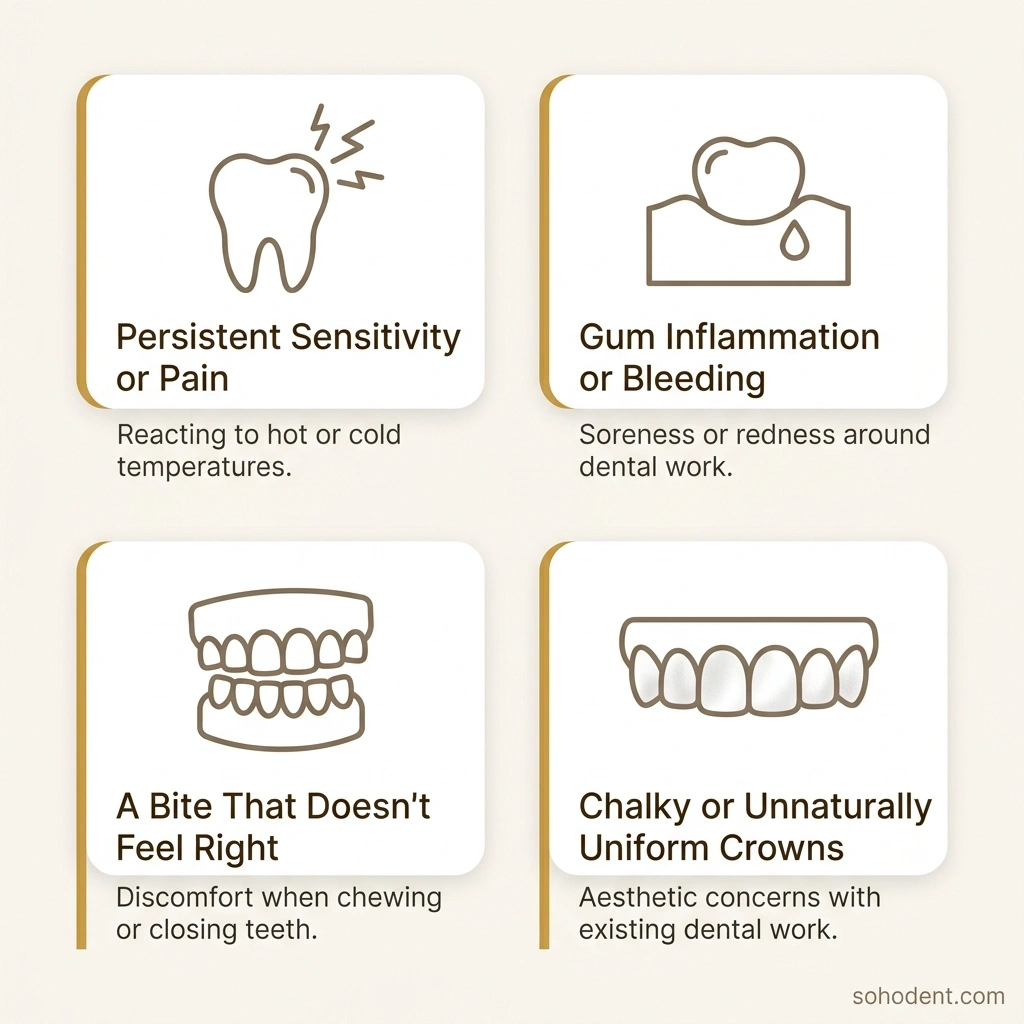
When a tooth is cut down aggressively to fit a crown, the nerve inside can become inflamed or, in more serious cases, permanently damaged. The result is a tooth that throbs, aches when you bite, or reacts sharply to temperature weeks or months after the work was finished — on a tooth that was healthy before treatment. This usually means the tooth needs root canal treatment, or in rarer cases, extraction.
Crowns that don't sit flush against the gumline — either too bulky or with an open margin — trap plaque in a spot you can't clean properly with a toothbrush. Over weeks, this shows up as gums that bleed easily, look swollen, or gradually recede, revealing a dark line where the crown meets the tooth. This is a fitting problem, not something you're doing wrong at home.
When a full arch of crowns is fitted quickly, small differences in how the teeth meet are easy to miss without a careful bite check. Even a slightly high or uneven contact point can cause jaw pain, headaches, or cracked and chipped restorations further down the line, because the bite forces are landing unevenly every time you chew.
This is more of an aesthetic complaint than a health one, but it's one of the most common reasons patients feel their treatment "went wrong." Monolithic zirconia — a strong, solid-colour ceramic — is sometimes used across an entire smile because it's faster and cheaper to produce, even when a patient wanted the light-reflecting, layered look of a material like E-max. The result is teeth that look flat, overly white, and slightly artificial under normal lighting.
Manufacturing a full arch of crowns as one connected piece — rather than as individual crowns — is a faster and cheaper way to deliver a large case. It comes with real downsides: it's harder to clean between "teeth" that are actually joined together, which drives gum inflammation, and if one section chips or fails, the whole splinted piece often needs replacing rather than just the affected tooth.
| ⚠ When to see a dentist sooner rather than later: a tooth that throbs or darkens, a crown that has visibly lifted or separated, swelling that is increasing rather than settling, or a bite that has changed noticeably since the appointment. None of these need to be an emergency — but none of them improve by waiting. |






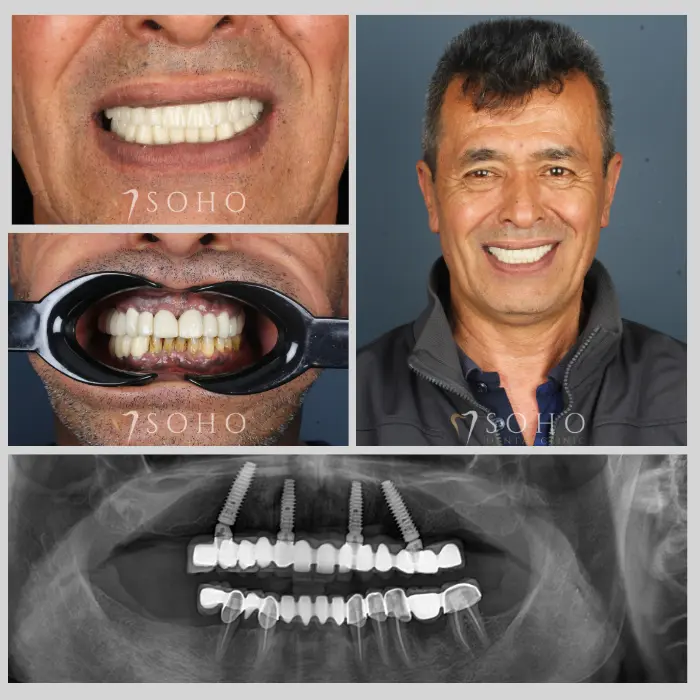
Everything above applies to veneers and crowns — restorations placed on your natural teeth. Implants are a different structure entirely: a titanium post fused into the jawbone, with its own separate set of failure signs (persistent pain around the implant site, visible movement, or a crown that has come loose from the post underneath) and a very different repair process involving bone healing rather than a simple remake.
If your concern is around a dental implant or a full-arch case like All-on-4 rather than a crown or veneer, our detailed guide on implant failure and revision surgery covers those warning signs and what a proper rescue treatment involves.
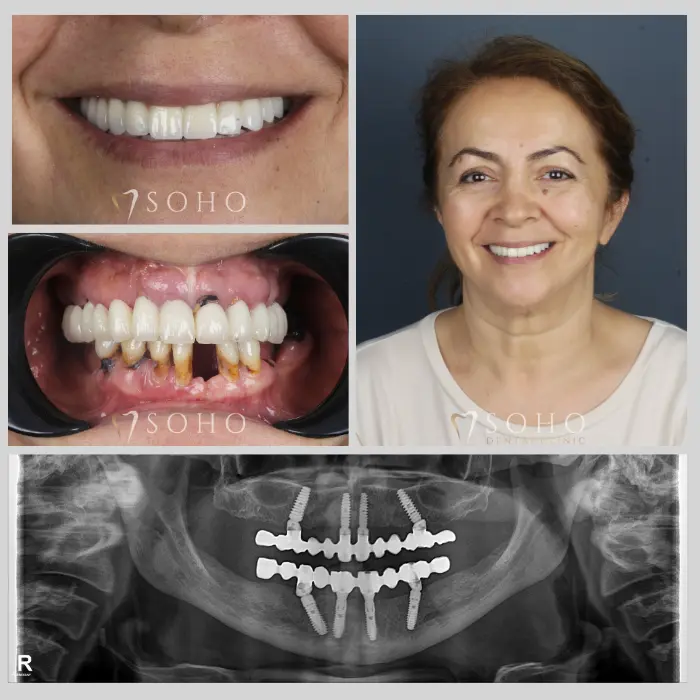
In most cases, yes — but the right first step is a proper, tooth-by-tooth reassessment, not another full-arch package. That means X-rays to check the health of the nerve and the bone underneath, a close look at how each crown or veneer actually fits at the gumline, and a bite check to see whether the way your teeth meet needs correcting. A good clinic will tell you honestly which teeth are fine as they are, which restorations need remaking, and which — if any — need more involved treatment such as root canal therapy.
If teeth have already been reduced for crowns, going back to something more conservative like a veneer usually isn't possible — there often isn't enough of the original tooth left to support it. The realistic path is a well-made, well-fitted crown replacing the poorly made one, not a step backward to a less invasive treatment. This is why the first decision — veneer versus crown — matters so much, and why a careful reassessment before doing anything further is worth the time.
When a patient comes to us with a previous crown or veneer case that isn't working, we don't start by proposing another full-arch package. We start with digital scans and X-rays of the teeth actually involved, so we can see the condition of each nerve and each gum margin individually — not guess from a photo. From there, each tooth is assessed on its own: some may only need a better-fitted crown, some may need gum treatment first to calm inflammation before any new restoration is placed, and a small number may need root canal treatment if the nerve has already been affected. Material choice is discussed openly — if the earlier "chalky" or overly uniform look was the concern, we talk through where a more light-reflecting material such as E-max is a better fit, and where a stronger option like zirconium crown is the right call for a back tooth taking heavier bite force. Crowns are made and fitted individually rather than splinted together, specifically so that gum health and hygiene are easier to maintain and a single problem tooth can be corrected without touching the rest.
| What Went Wrong Before | Our Approach to the Correction |
|---|---|
| Crowns placed without checking if a veneer would have done the job | Tooth-by-tooth assessment first — only teeth that genuinely need a crown get one |
| Crowns splinted together as one piece | Crowns made and fitted individually, for hygiene and easier future repairs |
| One flat, opaque material used across the whole smile | Material matched to the tooth and to the look the patient actually wants (E-max vs. zirconium) |
| No bite check before permanent bonding | Bite checked and adjusted before anything is permanently fitted |
At Soho Dental Clinic, this reassessment can begin remotely: send us your photographs, and where available, your existing X-rays, and our team will give you an honest, tooth-by-tooth view of what's actually going on before you commit to anything. You can review our dental veneers and zirconium crown treatment pages for how we approach these cases, and our current price list for a transparent, per-item breakdown rather than a single bundled figure.









| If you're unsure whether what you're seeing is normal or not, a second opinion costs nothing at Soho Dental. Send us your photos for a free, no-obligation review → |

Most of the discomfort in the first couple of weeks after veneer or crown treatment is normal healing, not a warning sign. What matters is the trend: symptoms that are settling are probably fine; symptoms that are the same or worse a month or two later, or that only appear months down the line, deserve a proper look. A tooth-by-tooth reassessment — not another bundled package — is the right starting point if you're unsure.
 Dental Veneers
Dental Veneers